
DVT PROPHYLAXIS
Low risk: 40 mg SC Daily
High risk: 30 mg SC BID
BMI ≥ 40 kg/m2: 40 mg SC BID
High risk pregnant patients post- C-section delivery:
Patient weight < 90 kg: 40 mg SC Daily
Patient weight ≥ 90 kg: 40 mg SC BID
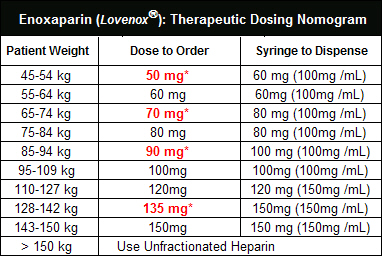
DVT/PE TREATMENT
1mg/kg* SC Q12H
UNSTABLE ANGINA / NSTEMI
Initial 30mg IV push (optional) followed by; 1mg/kg SC Q12H
(*Note: Patients weighing > 150 kg should use unfractionated heparin)
PERCUTANEOUS CORONARY INTERVENTION (PCI)
Prior Enoxaparin administration
³ 2 doses of 1mg/kg SC OR 30 mg IV bolus + 1mg/kg SC dose
If the last SC dose of Enoxaparin was given > 8 hours ago, administer an additional 0.3 mg/kg IV push
If the last 1 mg/kg SC dose of Enoxaparin was given < 8 hours ago, do not administer any additional doses
1 dose of SC with no IV bolus dose
Additional 0.3 mg/kg IV bolus at the time of PCI
No Prior Enoxaparin administration
With or without concurrent Glycoprotein IIb/IIIa inhibitors
0.5 - 0.75 mg/kg IV push
STEMI: (maximum of 8 days)
< 75 years: 30mg IV bolus followed by 1mg/kg SC Q12H
(Maximum 100mg for first 2 SC doses)
> 75 years: 0.75mg/kg SC Q12H (Maximum 75mg/dose for first 2 SC doses)
ENOXAPARIN DOSING ACCORDING TO RENAL FUNCTION
**** Not recommended in acute renal failure, ESRD or dialysis ****
CrCl <30 mL/minute:
DVT prophylaxis in abdominal surgery, hip replacement, knee replacement, or in medical patients during acute illness: 30 mg once daily
DVT treatment (inpatient or outpatient treatment in conjunction with warfarin): 1 mg/kg once daily
STEMI, Unstable angina, NSTEMI: 1 mg/kg once daily
REVERSAL OF ENOXAPARIN EFFECTS
Protamine sulfate: partial reversal ~55% of anti-Xa activity
If ≤ 8 hours since last dose: 1 mg protamine IV for every 1 mg of enoxaparin. A second infusion of 0.5 mg protamine for every 1 mg enoxaparin may be administered 2-4 hours after first infusion of protamine.
If > 8 hours since last dose: consult hematology service, may give smaller doses of protamine
Refer to Protamine monograph for administration information
CONVERTING FROM IV HEPARIN INFUSION TO ENOXAPARIN
Stop Heparin infusion
Wait 0-60 minutes. If PTT is > 100, consider waiting 90 minutes.
Administer enoxaparin dose.
CONVERTING FROM ENOXAPARIN TO IV HEPARIN INFUSION
IV Heparin infusion with bolus may be initiated 12 hours after last Enoxaparin dose.
All listed syringes are graduated. (Prophylactic syringes: 30 mg & 40 mg are not graduated)
* How to administer (Partial or Dose Adjusted syringe)
Hold syringe upright (needle pointing up).
Expel air bubble and extra medication (verify correct dose).
Once at the correct dose, pull back plunger to add 0.1 mL air bubble (air bubble ensures dose will be completely administered).
Select site for subcutaneous injection and administer

Rev: September 2012